Removable Partial Denture: Clasps
On 05 Oct 2020 | Read time about 4 Minutes
On This Page
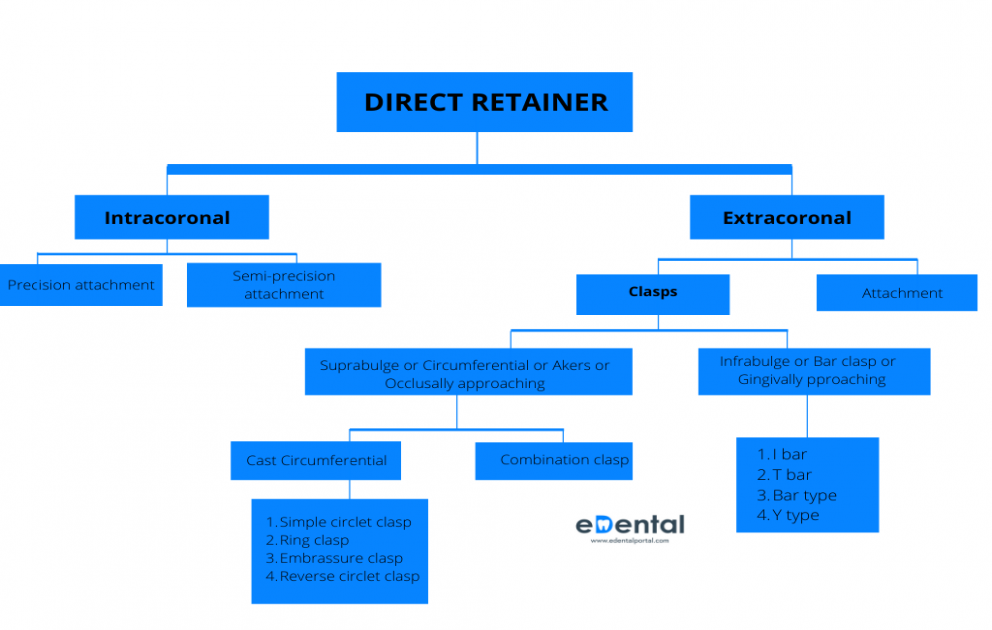
Direct retainer is a component of removal partial dentures (RPD), which is used to retain and prevent dislodgement, consisting of a clasp assembly or precision attachment. Depending on their placement inside (within) the abutment tooth or outside (surrounding) the abutment, direct retainers can be broadly classified as:
- Intracoronal
- Extracoronal

Clasps
Types of Clasps
- Suprabulge (originate above the survey line) or Occlusally approaching clasp or Circumferential or Akers Clasp
- Infrabulge (originate below the survey line) or Gingivally approaching clasp or Bar Clasp
Types of Suprabulge or Occlusally approaching clasps
Simple circlet clasp
- Widely used clasp
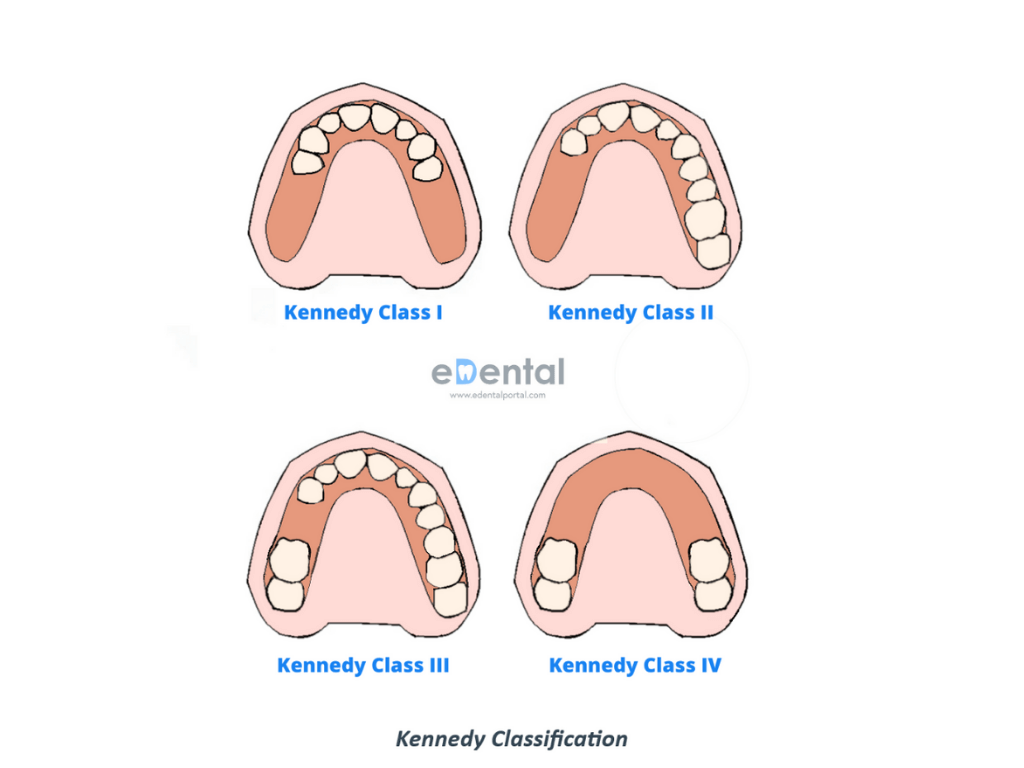
- Clasp of choice in tooth supported RPD. E.g: Kennedy Class III

Ring Clasp
- Encircles nearly the entire abutment tooth
- Covers a large area of tooth surface, therefore requiring meticulous hygiene
- Mostly indicated in tipped mandibular molar

Embrasure clasp
This design is most frequently used in cases of unilateral edentulous span of an unmodified Kennedy Class II or Class III partial denture, on the side of the arch where there is no edentulous space.

Combination clasp
A combination clasp is a circumferential retainer for a removable dental prosthesis that has a cast reciprocal arm and a wrought wire retentive clasp (GPT8).
It consists of a wrought wire retentive arm and a cast reciprocal arm.
The combination of a wrought alloy and cast alloy gives it the name ‘combination clasp’.
- It is indicated on an abutment adjacent to a distal extension base where only a mesiobuccal undercut exists on the abutment.
- It is used when maximum flexibility is desirable, such as on an abutment tooth adjacent to a distal extension base or where a large tissue undercut or on a weak abutment when a bar-type direct retainer is contraindicated.
The patient may be taught to avoid distortion of the wrought wire by explaining how to remove a partial denture- the fingernail should always be applied to its point of origin, where it is held rigid by the casting, rather than to the flexible terminal end. Often, lingual retention may be used rather than buccal retention, especially on a mandibular abutment, so that the patient never touches the wrought- wire arm during removal of the denture. Instead, removal may be accomplished by lifting against the cast reciprocal arm located on the buccal side of the tooth.

Infrabulge (originate above the survey line) or Gingivally approaching clasp or Bar Clasp
These clasps are named infrabulge or gingivally approaching clasp since it approaches the undercut areas from gingival direction.
Tooth and tissue born situations (Kennedy Class I & II) requires special attention in direct retainer selection, due to stresses created by rotational movements of the prostheses. When the denture bases are placed under function, rotation occurs about the rest seats of the most posterior abutments.
Excessive occlusal forces on the distal-extension portion of the denture could cause a torqueing action on the abutment teeth unless direct retainers are designed with stress-breaking capabilities. Stress releasing clasp assemblies include:
• The bar clasp with mesial rest (e.g.RPI)
• The RPA clasp
• The combination clasp
Bar clasp with mesial rest
The RPI is a current concept of bar clasp design that refers to the rest, proximal plate, and I-bar component parts of the clasp assembly.
- Small undercut (0.01 inch) existing in cervical third of abutment
- Distal extension abutments to engage a distobuccal (adjacent to edentulous space) undercut.
- Most tooth-supported partial dentures including modification spaces where aesthetics is a concern.
The bar clasp arm has been classified by the shape of the retentive terminal. Thus it has been identified as a T, modified T, I, or Y. The form the terminal takes is of little significance as long as it is mechanically and functionally effective, covers as little tooth surface as possible, and displays as little metal as possible.

RPA:
This concept includes the rest, proximal plate and Akers (RPA) clasps.
If the abutment teeth demonstrate contraindications for a bar-type clasp (i.e., exaggerated buccal or lingual tilts, severe tissue undercut, or a shallow buccal vestibule) and the desirable undercut is located in the gingival third of the tooth away from the extension base area, a modification should be considered for the RPI system (the RPA clasp).

Clasp selection is critical only when abutment tooth is adjacent to distal extension base. If mesiobuccal undercut is present – combination clasp is used, if distobuccal undercut is present – bar clasp is used. If bar clasp is contraindicated, a reverse circlet clasp is used.
Reverse circlet clasp is indicated in distal extensions (Kennedy Class I and Class II) when distobuccal undercut is present. As the denture base moves down, the clasp moves further gingivally into the undercut without contacting the abutment. The clasp may produce wedging force between the abutment and the adjacent tooth, which can be countered by preparing a distal occlusal rest on the adjacent teeth also (To protect the marginal ridge, an additional rest must be placed adjacent to edentulous space, which will decrease the releasing action of the clasp tip).
Reverse circlet clasp often gives a poor esthetic result with excessive display of metal as clasp runs from mesial to distal side of facial surface, hence is not the choice in premolars.
On This Page
Latest Posts




FREE PROMETRIC PRACTICE TESTS
Try out the most relevant Prometric mock test questions for Dental exams here.
ENROLL NOW



